
Diffuse Soft Tissue Mineralization in a Cat
Contributer: C. GantaHistory: A five month old female domestic short hair cat had chronic cough which was non-responsive to antibiotics or vaccines. Tracheal wash bacterial culture was negative, mycoplasma by PCR was negative and toxoplasma serology was negative.
Gross Lesions:
Lungs: The lungs failed to collapse and were white, firm, and crunchy.

Lungs, multifocal to coalescing areas of mineralization

Mineralized lung, cut section- most of the lung is affected
Aorta: The proximal 3 – 4 cm of the aorta and bracheocephalic trunk had multifocal areas of a hard, white, gritty material on the intimal surface. There were multiple small (2- 2.5mm diameter), round diverticula in the very proximal aorta.

Heart, aorta- multifocal mineralized plaques
Stomach: The serosal surface of the stomach was grayish white and firm. There was accentuation of the gastric rugae and the mucosa was rough and granular with diffuse mineralization. The distal esophagus also had multifocal 2-3 mm diameter circular mineral deposits on the mucosa.

Stomach- mucosal mineralization
Kidneys: The cortex of both kidneys was thin (about 3-4 mm), and contained mineral deposits with rough, gritty texture.

Kidney- diffuse cortical mineralization
Other lesions:
In the thoracic cavity the subpleural connective tissue had mild horizontal steaks of mineralization in the cranial intercostal spaces, giving a horizontal ladder like appearance. There was about 3 ml of reddish brown watery fluid in the pericardial sac. The eyes, brain, heart, skin, reproductive system, small and large intestines, and liver were all grossly normal.
Histopathology:
Lungs: Diffusely, the alveolar septae are mineralized and alveoli contained increased numbers of alveolar macrophages. The pulmonary aorta and bracheocephalic trunk contain multifocal deposits of mineral in the intima and media with complete loss of the endothelium.
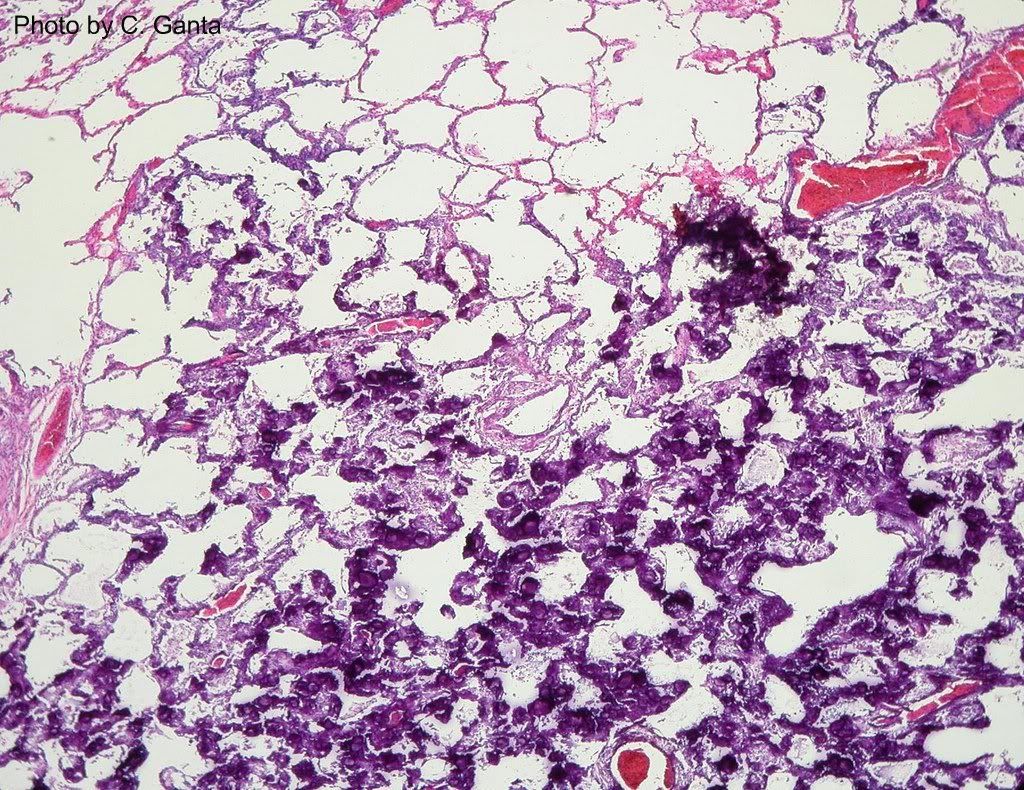
Lung- alveolar septae are mineralized
Stomach: There are multifocal to coalescing areas of mineralization within the middle and deep mucosa, lamina propria, submucosa and muscularis.

Stomach- the mucosa in diffusely mineralized
Aorta: Within the lamina propria and submucosa the arteriolar intima and media are replaced by mineral deposits.

Aorta- mineralization of the intima and muscular layer
Kidneys: Within the cortex the there is mineralization of the tubular basement membranes, interstitium, Bowman’s capsule and blood vessels with tubular loss and interstitial fibrosis. Diffusely, the glomeruli are arborized with a few immature glomeruli.
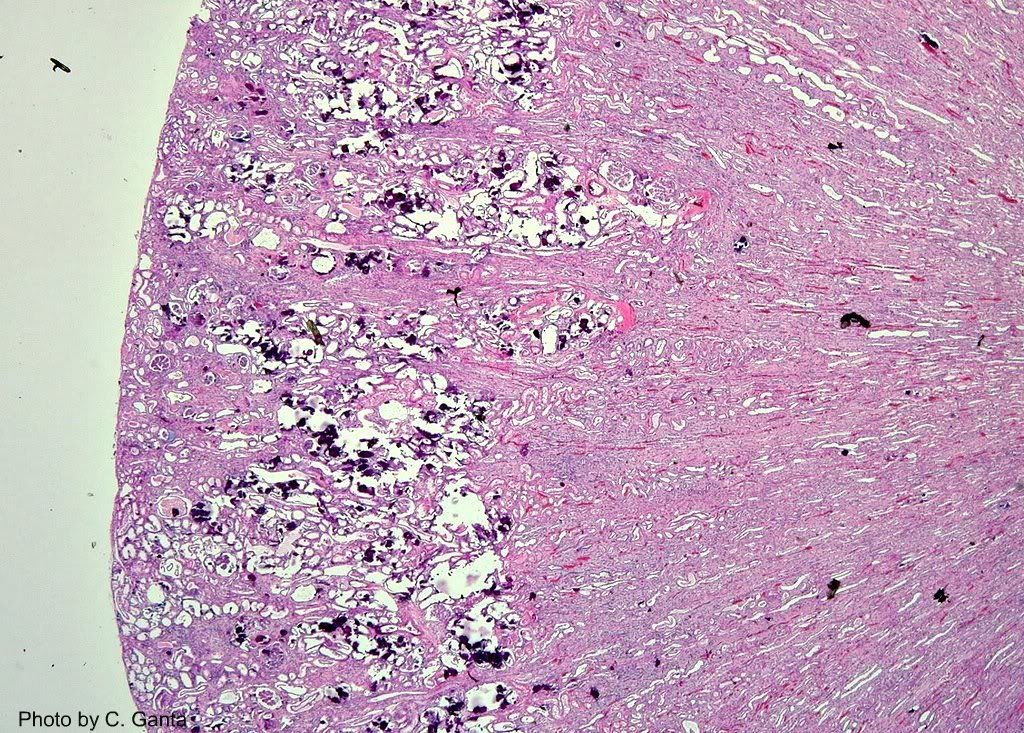
Kidney- extensive cortical mineralization including Bowmans capsule and tubules
There are no microscopic lesions in esophagus, liver, spleen, thyroid, parathyroid, adrenal glands, lymph nodes, urinary bladder and brain.
Comment:
A serum chemistry prior to death showed very high levels of calcium and phosphorus but normal levels of creatinine and moderately high levels of blood urea nitrogen. The increased serum levels of calcium and phosphorus with no indication of renal failure was suggestive of chronic vitamin D toxicosis.
Excess vitamin D and its active metabolites will increase the absorption of calcium and phosphorus from the intestines. The level of calcium absorption from the intestine is dependant on the serum levels of calcium binding protein (CBP) which is usually elevated in excess vitamin D. The excess amount of calcium and phosphorus in the serum will precipitate in the lungs, kidneys, aorta, gastric mucosa and submucosa among others.



interesting…..